Questions that need to be addressed when treating endometriomas on the ovary
1. How old is the woman
2. Has there been previous surgery for ovarian endometriosis
3. What symptoms is the cyst causing
4. Is fertility an immediate issue
5. If fertility is not an immediate issue what will be done to prevent recurrence
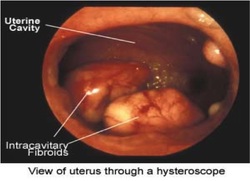
Endometriomas are ovarian cysts caused by endometriosis.
Most times they are as a result of adhesions between the pelvic sidewall and the ovary caused by endometriosis.
Endometriosis is characterized by symptoms of pain during periods (sometimes also when not having periods), and may also be implicated in infertility problems.
Most endometriomas are diagnosed on the basis of symptoms and results of an ultrasound scan
Because of what we now know about the effect of endometriomas on the ovary and its function, and the effects of surgery on future ovarian function, it is important the doctors treat each patient diagnosed individually taking into consideration:
1. The age of the patient
a. The age of the woman is important as over the age of 40 there may be increased relative risk of developing cancer of the ovary as a result of endometriosis
2. The life stage of the patient
a. Whether fertility is an immediate issue
b. Whether surgery has taken place already on the ovary
It is now thought that leaving the endometriomas on the ovary has a detrimental effect on the ovary. It can cause
1. Oxidative stress
2. Production of toxins that may harm the ovary
3. Reduction of the number of follicles
4. Increased fibrosis within the ovary
However treatment of the ovary may lead to
1. reduced AMH levels
a. AMH is a maker of ovarian reserve
2. Reduced response to ovarian stimulation if IVF is required
3. Premature ovarian failure in 2.4% of women after repeat operation depending on age
For these reasons it is important to balance treatment of the endometriomas with considerations to prevent the endometriomas from coming back. (The risk of it coming back is in the region of about 12% after formal removal of the endometrioma. If it is only drained the risk of recurrence is about 100%).
1. How old is the woman
2. Has there been previous surgery for ovarian endometriosis
3. What symptoms is the cyst causing
4. Is fertility an immediate issue
5. If fertility is not an immediate issue what will be done to prevent recurrence
Endometriomas are ovarian cysts caused by endometriosis.
Most times they are as a result of adhesions between the pelvic sidewall and the ovary caused by endometriosis.
Endometriosis is characterized by symptoms of pain during periods (sometimes also when not having periods), and may also be implicated in infertility problems.
Most endometriomas are diagnosed on the basis of symptoms and results of an ultrasound scan
Because of what we now know about the effect of endometriomas on the ovary and its function, and the effects of surgery on future ovarian function, it is important the doctors treat each patient diagnosed individually taking into consideration:
1. The age of the patient
a. The age of the woman is important as over the age of 40 there may be increased relative risk of developing cancer of the ovary as a result of endometriosis
2. The life stage of the patient
a. Whether fertility is an immediate issue
b. Whether surgery has taken place already on the ovary
It is now thought that leaving the endometriomas on the ovary has a detrimental effect on the ovary. It can cause
1. Oxidative stress
2. Production of toxins that may harm the ovary
3. Reduction of the number of follicles
4. Increased fibrosis within the ovary
However treatment of the ovary may lead to
1. reduced AMH levels
a. AMH is a maker of ovarian reserve
2. Reduced response to ovarian stimulation if IVF is required
3. Premature ovarian failure in 2.4% of women after repeat operation depending on age
For these reasons it is important to balance treatment of the endometriomas with considerations to prevent the endometriomas from coming back. (The risk of it coming back is in the region of about 12% after formal removal of the endometrioma. If it is only drained the risk of recurrence is about 100%).












 RSS Feed
RSS Feed