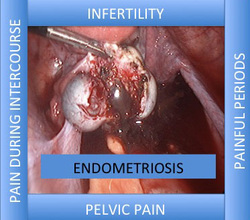
Endometriosis affects 20-40% of women with infertility against a background risk of 5-10% of women in the general population. Thus endometriosis can be responsible in some cases for failure to conceive.
It is thought that endometriosis can cause infertility by
· Making sexual intercourse painful thus women avoid having intercourse (dyspareunia)
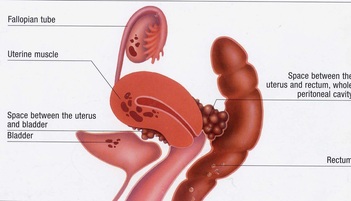
· Altering the pelvic anatomy making it difficult for the sperm and the egg to meet (interfering with fertilization)
· Interfere with the development of the embryo (after the sperm and egg have met)
· Interfering with implantation. Interfering with the process by which the embryo embeds itself in the womb
Endometriosis is staged from stage I- 4, and though the actual stage does not determine the ability to get pregnant or symptoms that women have, it is used by doctors and carers to give a possible prognosis and outcome of treatment.
Stage I is minimal disease whilst stage 4 is severe disease
For women who want to get pregnant with endometriosis
It is first important that the male partner have a sperm test to ensure that the semen is of acceptable standard to achieve pregnancy.
A pelvic ultrasound scan is usually performed as this will help find out whether there are any cysts associated with endometriosis and on occasion can determine the severity of the disease.
If doctors feel that the disease is severe they will ask for other tests.
For women with mild pain symptoms treatment with painkillers may be all that is required and doctors will advise them to try and get pregnant naturally.
Other forms of medical management with hormones are not compatible with fertility.
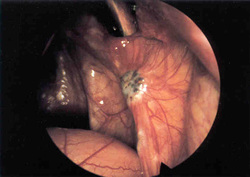
For women who have more pain a laparoscopy is usually required.
The aim of the laparoscopy would be
1. To diagnose the disease
2. To stage the disease
3. To debulk the disease
a. To remove all visible disease
4. Restore anatomy
5. Test tubal patency
With superficial/minimal endometriosis medical studies have shown that removing the disease improves pregnancy rates in women with endometriosis. One particular study showed a 2 fold increase in fertility rates, however when the study was pooled with other existing data the effect was not that great, the number needed to treat to improve fertility for one person was about 8.
The treatment effect on women with more severe endometriosis is not that clear, however treatment has been shown to improve pain symptoms and thus increase the frequency of intercourse in women who suffered from difficulty with intercourse, thus potentially improving fertility.
In women with ovarian endometriosis (endometriomas) the general advice is to get them treated. This is usually done by laparoscopy. Some medical studies show that removing these cysts can improve pregnancy rates by up to 50%. It also improve painful sex in women who suffer from dyspareunia and painful periods
Removal of the cyst is usually advised as opposed to just drainage of the cyst as this reduces the risk of recurrence.
The recurrence risk is nearly 100% if the cysts are only drained as opposed to removed where the recurrence risk is less than 10%
A more complete assessment is required for women in whom the cysts recur as repeated operations for endometriomas may reduce ovarian reserve and adversely affect pregnancy rates
In relation to IVF there is still great medical debate, but most would suggest that endometriomas larger than 4cm should be treated prior to IVF.
For most women it is best that they be seen to endometriosis experts in endometriosis centers as this optimizes treatment and reduces the risk of recurrence.
It is thought that endometriosis can cause infertility by
· Making sexual intercourse painful thus women avoid having intercourse (dyspareunia)
· Altering the pelvic anatomy making it difficult for the sperm and the egg to meet (interfering with fertilization)
· Interfere with the development of the embryo (after the sperm and egg have met)
· Interfering with implantation. Interfering with the process by which the embryo embeds itself in the womb
Endometriosis is staged from stage I- 4, and though the actual stage does not determine the ability to get pregnant or symptoms that women have, it is used by doctors and carers to give a possible prognosis and outcome of treatment.
Stage I is minimal disease whilst stage 4 is severe disease
For women who want to get pregnant with endometriosis
It is first important that the male partner have a sperm test to ensure that the semen is of acceptable standard to achieve pregnancy.
A pelvic ultrasound scan is usually performed as this will help find out whether there are any cysts associated with endometriosis and on occasion can determine the severity of the disease.
If doctors feel that the disease is severe they will ask for other tests.
For women with mild pain symptoms treatment with painkillers may be all that is required and doctors will advise them to try and get pregnant naturally.
Other forms of medical management with hormones are not compatible with fertility.
For women who have more pain a laparoscopy is usually required.
The aim of the laparoscopy would be
1. To diagnose the disease
2. To stage the disease
3. To debulk the disease
a. To remove all visible disease
4. Restore anatomy
5. Test tubal patency
With superficial/minimal endometriosis medical studies have shown that removing the disease improves pregnancy rates in women with endometriosis. One particular study showed a 2 fold increase in fertility rates, however when the study was pooled with other existing data the effect was not that great, the number needed to treat to improve fertility for one person was about 8.
The treatment effect on women with more severe endometriosis is not that clear, however treatment has been shown to improve pain symptoms and thus increase the frequency of intercourse in women who suffered from difficulty with intercourse, thus potentially improving fertility.
In women with ovarian endometriosis (endometriomas) the general advice is to get them treated. This is usually done by laparoscopy. Some medical studies show that removing these cysts can improve pregnancy rates by up to 50%. It also improve painful sex in women who suffer from dyspareunia and painful periods
Removal of the cyst is usually advised as opposed to just drainage of the cyst as this reduces the risk of recurrence.
The recurrence risk is nearly 100% if the cysts are only drained as opposed to removed where the recurrence risk is less than 10%
A more complete assessment is required for women in whom the cysts recur as repeated operations for endometriomas may reduce ovarian reserve and adversely affect pregnancy rates
In relation to IVF there is still great medical debate, but most would suggest that endometriomas larger than 4cm should be treated prior to IVF.
For most women it is best that they be seen to endometriosis experts in endometriosis centers as this optimizes treatment and reduces the risk of recurrence.








 RSS Feed
RSS Feed