This treatment is a safe and effective alternative to surgery for some women who suffer from symptoms related to uterine fibroids. This method of treatment that does not require an operation was first reported in 1996.
80% of women find relief of their symptoms, and the fibroids shrink by about 40% in volume.
It is less invasive than myomectomy or hysterectomy for the treatment of symptoms of fibroids, and in the short term it is associated with a shorter hospital stay and return to normal activities
Is it suitable for all fibroids?
It is best suited for fibroids that are located in the muscle of the womb. It is less suitable for fibroids that have developed stalks and are attached by these stalks to the uterus (pedunculated fibroids), as sometimes when this type of fibroid is deprived of blood supply by the embolization process, they may drop off onto bowel and become necrotic and cause complications.
Who performs the procedure?
Interventional radiologists perform the procedure.
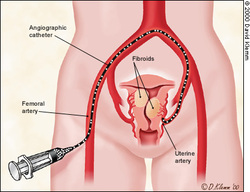
How is the procedure performed?
A general anaesthetic is not required for this procedure. A catheter is inserted into the femoral artery (a major vessel in the groin area) after local has been used to numb the crease of the groin. X-ray guidance (fluoroscopy) is used to manipulate the catheter until it gets to the uterine artery (the major vessel that supplies the womb and the fibroids). The aim is to block off the blood supply to the fibroid. Once the blood supply of the fibroid has been identified special particles are used to effect blockage. The procedure usually takes the best part of 45 minutes.
After effects of the procedure
The procedure can be painful thus all women are usually given painkillers for the procedure.
After the procedure for a week or two women may have flu like symptoms (post-embolization syndrome) but these usually pass with the use of painkillers and anti-inflammatory agents. For this reason though the symptoms may regress in the first few days it is best to plan a week or maybe 2 off work
There may be a vaginal discharge, for the first few weeks, which also gets better over time but may persist in about 16% of women for up to a year.
Some women may notice that they pass one or more of their fibroids vaginally (fibroid expulsion). This is usually of little consequence, but if it still attached to the womb by a stalk and cannot detach itself, an additional procedure may be required to remove the fibroid this happens in about 6-10% of women and is usually within 6 months of the procedure.
Embolisation can result in infection in about 0.5% of cases most of which settle with a course of antibiotics. In the extremis it can result in septicemia necessitating emergency hysterectomy as a life-saving procedure.
Embolization is contraindicated in women who have active pelvic infection
80% of women find relief of their symptoms, and the fibroids shrink by about 40% in volume.
It is less invasive than myomectomy or hysterectomy for the treatment of symptoms of fibroids, and in the short term it is associated with a shorter hospital stay and return to normal activities
Is it suitable for all fibroids?
It is best suited for fibroids that are located in the muscle of the womb. It is less suitable for fibroids that have developed stalks and are attached by these stalks to the uterus (pedunculated fibroids), as sometimes when this type of fibroid is deprived of blood supply by the embolization process, they may drop off onto bowel and become necrotic and cause complications.
Who performs the procedure?
Interventional radiologists perform the procedure.
How is the procedure performed?
A general anaesthetic is not required for this procedure. A catheter is inserted into the femoral artery (a major vessel in the groin area) after local has been used to numb the crease of the groin. X-ray guidance (fluoroscopy) is used to manipulate the catheter until it gets to the uterine artery (the major vessel that supplies the womb and the fibroids). The aim is to block off the blood supply to the fibroid. Once the blood supply of the fibroid has been identified special particles are used to effect blockage. The procedure usually takes the best part of 45 minutes.
After effects of the procedure
The procedure can be painful thus all women are usually given painkillers for the procedure.
After the procedure for a week or two women may have flu like symptoms (post-embolization syndrome) but these usually pass with the use of painkillers and anti-inflammatory agents. For this reason though the symptoms may regress in the first few days it is best to plan a week or maybe 2 off work
There may be a vaginal discharge, for the first few weeks, which also gets better over time but may persist in about 16% of women for up to a year.
Some women may notice that they pass one or more of their fibroids vaginally (fibroid expulsion). This is usually of little consequence, but if it still attached to the womb by a stalk and cannot detach itself, an additional procedure may be required to remove the fibroid this happens in about 6-10% of women and is usually within 6 months of the procedure.
Embolisation can result in infection in about 0.5% of cases most of which settle with a course of antibiotics. In the extremis it can result in septicemia necessitating emergency hysterectomy as a life-saving procedure.
Embolization is contraindicated in women who have active pelvic infection









 RSS Feed
RSS Feed