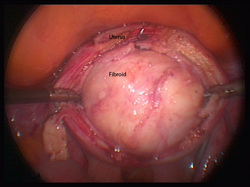
Below is a video showing a large broad ligament fibroid (in an awkward position) being removed by keyhole surgery. The important thing is careful surgical technique, and the use of substances to reduce blood loss and to help prevent the development of scar tissue.
Having fibroids removed is a major undertaking both for the surgeon and the patient. The method of operation will depend on the number and size of the fibroids and how the fibroids are related to the womb.
Traditionally all fibroids were removed by open surgery but increasingly it is now possible to operate on fibroids laparoscopically (using “keyhole surgery), though size, number and site of the fibroids is taken into consideration it is possible to operate and large, “awkwardly” located and numerous fibroids by means of keyhole surgery.
Irrespective of the type of surgery there are complications that should be considered, this is what I tell all patients who are having a myomectomy:
Just because the fibroids are there does not mean you have to remove them the only reason for removal is to improve symptoms.
Removing fibroids is not a sport
There are reports of more than 200 fibroids being removed from one individual. On occasion this may be necessary but I will remove fibroids that are causing symptoms with the aim to improve fertility. I will not continue just because I can if I feel that the womb will be too scarred it may on occasion be necessary to leave some behind
Things you need to consider before you go ahead
1. Adhesions (scar tissue formation after surgery)
Most women who have fibroids removed will develop adhesions (scar tissue that is a consequence of tissue healing). The quoted figure is about 90% however this can be halved with laparoscopic surgery. Measures to prevent the development of adhesions should be used during fibroid surgery.
Adhesions can lead to:
a. Problems with fertility
b. Problems with chronic pelvic pain
c. Problems with intestinal obstruction
It is important to ask your doctor what type of adhesion prevention will be used during your surgery
2. Blood Transfusion:
Fibroid operations are potentially bloody operations; most women who have these operations will bleed. The risk of a blood transfusion ranges from 1 in 20 to 1 in 50 depending on the size of the fibroid, the number of fibroids and their location.
There are surgical techniques that are used to decrease bleeding including temporary tourniquets.
There are also medications that are used to decrease the risk of bleeding these include:
a. Vasopressin
b. Misoprostol
c. GnrH analogues like Zoladex. I prefer not to use this particular drug unless my patients are anaemic as women in whom it is used preoperatively are at greater risk of fibroid regrowth after myomectomy.
For women who want to avoid blood transfusions “cell-savers” where own blood is filtered and used for transfusion can be used.
Ask your doctor about these issues before you proceed with surgery.
Traditionally all fibroids were removed by open surgery but increasingly it is now possible to operate on fibroids laparoscopically (using “keyhole surgery), though size, number and site of the fibroids is taken into consideration it is possible to operate and large, “awkwardly” located and numerous fibroids by means of keyhole surgery.
Irrespective of the type of surgery there are complications that should be considered, this is what I tell all patients who are having a myomectomy:
Just because the fibroids are there does not mean you have to remove them the only reason for removal is to improve symptoms.
Removing fibroids is not a sport
There are reports of more than 200 fibroids being removed from one individual. On occasion this may be necessary but I will remove fibroids that are causing symptoms with the aim to improve fertility. I will not continue just because I can if I feel that the womb will be too scarred it may on occasion be necessary to leave some behind
Things you need to consider before you go ahead
1. Adhesions (scar tissue formation after surgery)
Most women who have fibroids removed will develop adhesions (scar tissue that is a consequence of tissue healing). The quoted figure is about 90% however this can be halved with laparoscopic surgery. Measures to prevent the development of adhesions should be used during fibroid surgery.
Adhesions can lead to:
a. Problems with fertility
b. Problems with chronic pelvic pain
c. Problems with intestinal obstruction
It is important to ask your doctor what type of adhesion prevention will be used during your surgery
2. Blood Transfusion:
Fibroid operations are potentially bloody operations; most women who have these operations will bleed. The risk of a blood transfusion ranges from 1 in 20 to 1 in 50 depending on the size of the fibroid, the number of fibroids and their location.
There are surgical techniques that are used to decrease bleeding including temporary tourniquets.
There are also medications that are used to decrease the risk of bleeding these include:
a. Vasopressin
b. Misoprostol
c. GnrH analogues like Zoladex. I prefer not to use this particular drug unless my patients are anaemic as women in whom it is used preoperatively are at greater risk of fibroid regrowth after myomectomy.
For women who want to avoid blood transfusions “cell-savers” where own blood is filtered and used for transfusion can be used.
Ask your doctor about these issues before you proceed with surgery.









 RSS Feed
RSS Feed