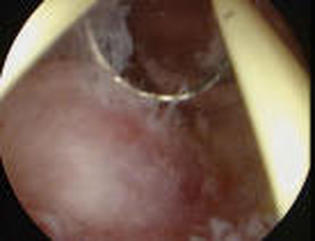
Video showing hysteroscopic resection of submucous fibroid
This is the second part of my post: Do fibroids forbid fertility.
Submucous fibroids can cause infertility, increase chances of miscarriage and complicate pregnancy.
Surgery is not always necessary for submucous fibroids, but for those implicated in infertility there is no rationale or evidence for medical management (treatment other than surgery)
Medical management involves the use of hormones. The only place for medical management for these fibroids is to shrink them before surgery. Shrinking the fibroids may make the operation easier for the surgeon and reduce the risk of some complications.
Sometimes if a woman is anaemic, hormones may be necessary to stop menstrual bleeding in order to improve the blood count in conjunction with iron therapy to prepare and optimize the body for surgery.
Most submucous fibroids causing infertility are removed by means of Hysteroscopic resection.
Hysteroscopic resection is where a small telescope (hysteroscope) is introduced into the uterine cavity. Attached to the hysteroscope is a wire loop, which is in turn attached to a high-energy electrical source. The instruments act like a “cheese wire” and allow the fibroids to be removed in a number of strips. Though it is possible to perform the procedure under local anaesthetic for small fibroids the majority require a general anaesthetic.
Factors that would influence my approach to the management of these fibroids would include the number of fibroids, the exact relationship of the fibroid to the uterine cavity and the size of the fibroid. As a general rule Hysteroscopic surgery is performed for no more than 3 fibroids with the largest being 5cm or less.
For larger submucous or deeper-seated submucous fibroids a 2-stage procedure may be necessary. In fact the deeper the fibroid is into the muscle of the uterus the more likely it will require more treatment. Only 9.7% of women with normal sized womb and no more than 2 submucous fibroids may need additional surgery, where as 35% of women will require additional surgery if the womb is enlarged and there are more than 3 submucous fibroids.
More recently especially for larger submucous fibroids and multiple submucous fibroids I use the laparoscopic approach. This is in keeping with recent literature that suggests this approach may have an advantage over Hysteroscopic surgery.
The theory behind this is that if a large area of the lining of the womb is removed with the Hysteroscopic procedure this may in it impair fertility.
P.S: If you have a question about this post, please leave a comment or share with your friends!
Submucous fibroids can cause infertility, increase chances of miscarriage and complicate pregnancy.
Surgery is not always necessary for submucous fibroids, but for those implicated in infertility there is no rationale or evidence for medical management (treatment other than surgery)
Medical management involves the use of hormones. The only place for medical management for these fibroids is to shrink them before surgery. Shrinking the fibroids may make the operation easier for the surgeon and reduce the risk of some complications.
Sometimes if a woman is anaemic, hormones may be necessary to stop menstrual bleeding in order to improve the blood count in conjunction with iron therapy to prepare and optimize the body for surgery.
Most submucous fibroids causing infertility are removed by means of Hysteroscopic resection.
Hysteroscopic resection is where a small telescope (hysteroscope) is introduced into the uterine cavity. Attached to the hysteroscope is a wire loop, which is in turn attached to a high-energy electrical source. The instruments act like a “cheese wire” and allow the fibroids to be removed in a number of strips. Though it is possible to perform the procedure under local anaesthetic for small fibroids the majority require a general anaesthetic.
Factors that would influence my approach to the management of these fibroids would include the number of fibroids, the exact relationship of the fibroid to the uterine cavity and the size of the fibroid. As a general rule Hysteroscopic surgery is performed for no more than 3 fibroids with the largest being 5cm or less.
For larger submucous or deeper-seated submucous fibroids a 2-stage procedure may be necessary. In fact the deeper the fibroid is into the muscle of the uterus the more likely it will require more treatment. Only 9.7% of women with normal sized womb and no more than 2 submucous fibroids may need additional surgery, where as 35% of women will require additional surgery if the womb is enlarged and there are more than 3 submucous fibroids.
More recently especially for larger submucous fibroids and multiple submucous fibroids I use the laparoscopic approach. This is in keeping with recent literature that suggests this approach may have an advantage over Hysteroscopic surgery.
The theory behind this is that if a large area of the lining of the womb is removed with the Hysteroscopic procedure this may in it impair fertility.
P.S: If you have a question about this post, please leave a comment or share with your friends!








 RSS Feed
RSS Feed